Neuroanatomy
Learning Objectives
- Define neuroanatomy and explain how it organizes the nervous system into clinically useful divisions.
- Identify the major components of the central and peripheral nervous systems.
- Describe the gross anatomy of the cerebrum, cerebellum, brainstem, spinal cord, meninges, and ventricles.
- Explain the functional importance of major tracts, cranial nerves, and autonomic pathways.
- Apply neuroanatomical principles to lesion localization using motor, sensory, reflex, and cranial nerve findings.
- Distinguish neuron types, glial support cells, and major patterns of white and gray matter organization.
Quick Answer
Neuroanatomy is the study of the structure of the nervous system and how those structures connect to function. It matters because neurological diagnosis is fundamentally anatomical. If a patient has facial weakness, aphasia, ptosis, hemiplegia, sensory loss, or an absent reflex, the next question is always: where is the lesion? The answer depends on understanding the brain, spinal cord, peripheral nerves, tracts, nuclei, meninges, and blood supply. Neuroanatomy can feel dense, but it becomes much easier when you treat it as a map for localization rather than a list of names.
Overview
The nervous system is broadly divided into:
- Central nervous system (CNS): brain and spinal cord
- Peripheral nervous system (PNS): cranial nerves, spinal nerves, ganglia, and peripheral nerves
Functionally, it includes:
- Somatic motor and sensory systems
- Autonomic pathways
- Higher cortical networks for language, memory, behavior, and planning
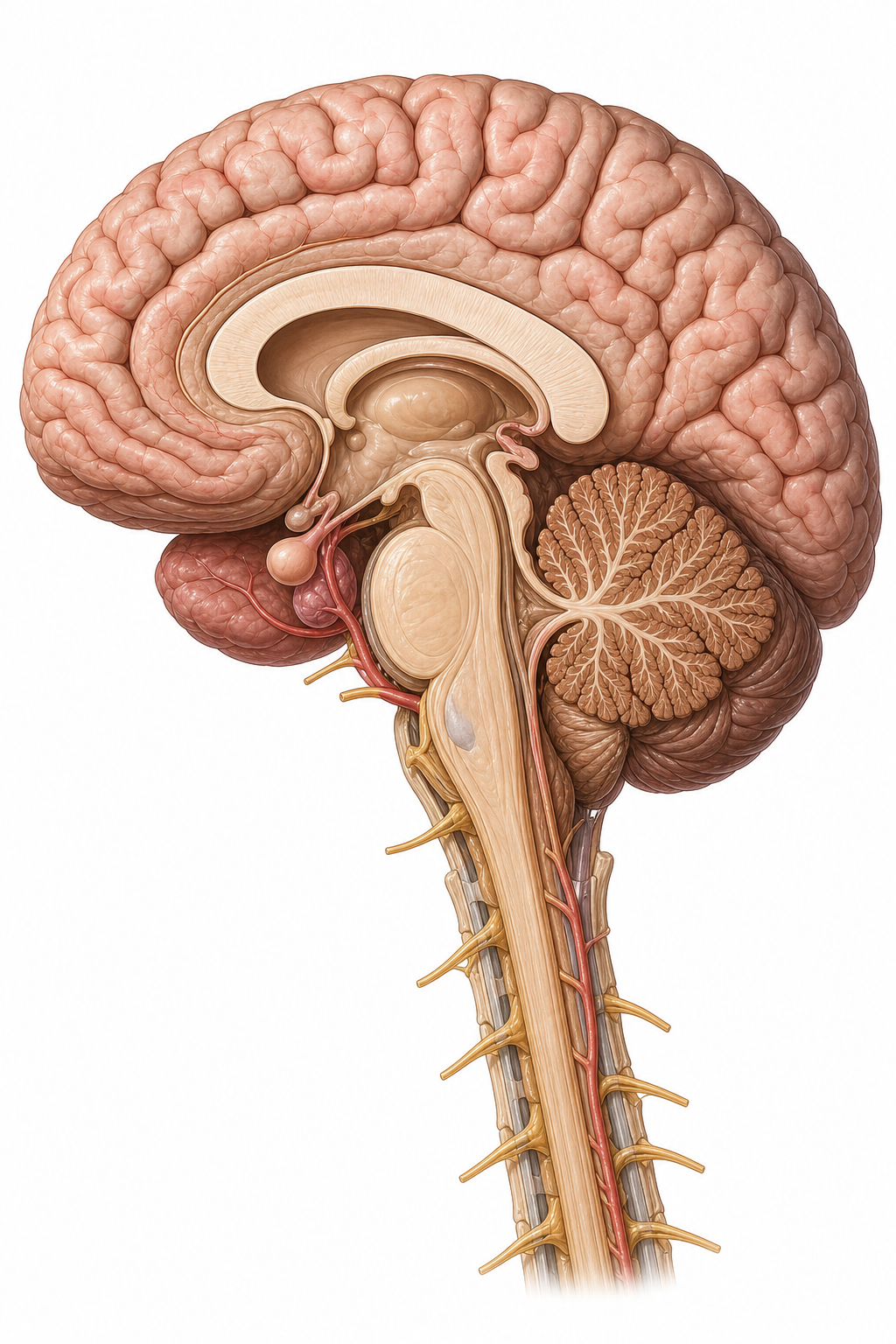
Figure 1. Start with this whole-system view so the cerebrum, cerebellum, brainstem, ventricular region, and cervical cord feel connected before you localize lesions.
Neurons and Glia
Neurons
Neurons are excitable cells that receive, process, and transmit information.
Main parts:
- Cell body
- Dendrites
- Axon
Neuroglia
| Cell Type | Main Role | Clinical Relevance |
|---|---|---|
| Astrocytes | Support and metabolic regulation | Gliosis, BBB support |
| Oligodendrocytes | Myelinate CNS axons | Multiple sclerosis |
| Schwann cells | Myelinate PNS axons | Peripheral nerve regeneration |
| Microglia | Immune surveillance | CNS inflammation |
| Ependymal cells | Line ventricles and central canal | CSF-related anatomy |
Why It Matters
Diseases often target support systems, not just neurons. Demyelinating disease is a classic example.
Common Misunderstanding
Students often treat glia as background cells. In reality, glial dysfunction can drive major neurological disease.
Central Nervous System
Cerebrum
The cerebrum contains two hemispheres and is responsible for conscious perception, voluntary movement, language, memory, and executive function.
Important lobes:
- Frontal
- Parietal
- Temporal
- Occipital
Cerebellum
Coordinates movement, balance, and motor learning.
Brainstem
Includes:
- Midbrain
- Pons
- Medulla
It contains vital autonomic centers and many cranial nerve nuclei.
Spinal Cord
The spinal cord transmits ascending sensory information and descending motor control while integrating reflexes.
Real-World Example
A lesion in the internal capsule can produce dense contralateral motor weakness because many descending fibers are tightly packed there.
Why It Matters
The more concentrated the pathways, the more dramatic the deficit from a small lesion.
Common Misunderstanding
Students often assume every brain region has only one function. Most regions participate in networks, but some lesion patterns are still highly localizing.
White Matter, Gray Matter, and Tracts
Gray Matter
Contains neuronal cell bodies, synapses, and processing centers.
White Matter
Contains myelinated axons connecting different regions.
Major Tracts
| Tract | Main Function | Lesion Clue |
|---|---|---|
| Corticospinal tract | Voluntary motor control | Weakness, hyperreflexia, Babinski sign |
| Dorsal columns | Fine touch, vibration, proprioception | Sensory ataxia, loss of vibration |
| Spinothalamic tract | Pain and temperature | Contralateral pain loss after crossing |
Example
Brown-Sequard syndrome demonstrates tract logic well: ipsilateral motor and vibration loss with contralateral pain and temperature loss below the lesion.

Figure 2. This labeled cross-section is the highest-yield visual for tract-based lesion localization and is worth revisiting during the practice-question section.
Brain Ventricles, CSF, and Meninges
Ventricular System
CSF flows through:
- Lateral ventricles
- Third ventricle
- Cerebral aqueduct
- Fourth ventricle
- Subarachnoid space
Meninges
- Dura mater
- Arachnoid mater
- Pia mater
Why It Matters
Hydrocephalus, meningitis, and intracranial hemorrhage are easier to understand once these layers and spaces are clear.
Real-World Example
An epidural hematoma is classically arterial and lies between skull and dura; a subdural hematoma lies beneath the dura and usually involves bridging veins.
Peripheral Nervous System
The PNS connects the CNS to muscles, glands, skin, and organs.
Spinal Nerves
Each spinal nerve carries sensory, motor, and autonomic fibers.
Cranial Nerves
Neuroanatomy overlaps strongly with head and neck anatomy here because cranial nerves carry special sensory and motor functions.
Autonomic Nervous System
- Sympathetic division: “fight or flight”
- Parasympathetic division: “rest and digest”
Clinical Localization Principles
Neuroanatomy becomes manageable when organized by localization questions.
Cortex or Brainstem?
- Aphasia suggests dominant cerebral cortex
- Crossed cranial nerve and body findings suggest brainstem
Spinal Cord or Peripheral Nerve?
- Sensory level and bilateral long tract signs suggest cord
- Distal pattern and reduced reflexes suggest peripheral nerve
UMN vs LMN
| Feature | Upper Motor Neuron Lesion | Lower Motor Neuron Lesion |
|---|---|---|
| Tone | Increased | Decreased |
| Reflexes | Increased | Decreased |
| Muscle bulk | Mild disuse atrophy | Marked atrophy |
| Fasciculations | No | Often present |
| Plantar response | Extensor may appear | Usually flexor/absent UMN signs |
Real-World Example
A patient with right facial droop sparing the forehead and right arm weakness likely has a left cortical or corticobulbar lesion rather than a peripheral facial nerve lesion.
Blood Supply and Stroke Relevance
Major cerebral circulation comes from:
- Internal carotid system
- Vertebrobasilar system
Important stroke territories:
- Middle cerebral artery
- Anterior cerebral artery
- Posterior cerebral artery
Why It Matters
Stroke symptoms often reflect vascular territory as much as anatomical structure.
Key Terms
| Term | Definition | Related Concept |
|---|---|---|
| Neuroanatomy | Study of nervous system structure | Lesion localization |
| CNS | Brain and spinal cord | Central processing |
| PNS | Nerves and ganglia outside CNS | Peripheral conduction |
| Gray matter | Area rich in neuronal cell bodies | Processing |
| White matter | Area rich in myelinated axons | Tracts |
| Corticospinal tract | Major descending motor pathway | UMN signs |
| Dorsal columns | Ascending pathway for vibration and proprioception | Sensory exam |
| Spinothalamic tract | Ascending pain and temperature pathway | Contralateral sensory loss |
| Meninges | Dura, arachnoid, pia | Meningitis, hemorrhage |
| Internal capsule | Dense white matter pathway region | Stroke deficits |
| Brainstem | Midbrain, pons, medulla | Cranial nerve nuclei |
| Ventricular system | CSF-containing spaces in brain | Hydrocephalus |
Common Mistakes
Misconception: Neuroanatomy is mostly memorization and has little direct clinical use.
Why it's wrong: Neurological examination is fundamentally anatomical and depends on localization.
Correct understanding: Neuroanatomy is one of the most clinically useful anatomy subjects because it explains symptom patterns.
Misconception: CNS and PNS diseases behave the same way because both involve nerves.
Why it's wrong: Myelination, regeneration potential, lesion signs, and supporting cells differ significantly between the CNS and PNS.
Correct understanding: Distinguishing central from peripheral pathology is a core neuroanatomical skill.
Misconception: If one side of the body is weak, the lesion must be in that same side of the brain.
Why it's wrong: Many motor pathways cross, so cortical and many brainstem lesions produce contralateral deficits.
Correct understanding: Always ask where the relevant pathway decussates before localizing a lesion.
Comparison and Connections
| Feature | Cerebral Cortex Lesion | Brainstem Lesion | Peripheral Nerve Lesion |
|---|---|---|---|
| Typical deficit pattern | Higher cortical dysfunction plus body deficit | Cranial nerve findings plus long tract signs | Distal or nerve-distribution weakness/sensory loss |
| Speech/language effects | Possible | Usually not primary aphasia | No |
| Reflex pattern | Often UMN | Often UMN below lesion | Often reduced |
| Example | MCA stroke | Lateral medullary syndrome | Radial nerve palsy |
Practice Questions
Recall
Q1. Name the main divisions of the CNS.
Answer guidance: Cerebrum, cerebellum, brainstem, and spinal cord.
Q2. Which glial cell myelinates axons in the CNS?
Answer guidance: Oligodendrocytes.
Understanding
Q3. Why can a small lesion in the internal capsule produce major weakness?
Answer guidance: Many descending motor fibers are tightly packed there.
Q4. Explain the basic difference between dorsal column and spinothalamic pathway function.
Answer guidance: Dorsal columns carry fine touch, vibration, and proprioception; spinothalamic tract carries pain and temperature.
Application
Q5. A patient has contralateral body weakness and forehead-sparing facial weakness. Where is the lesion likely?
Answer guidance: A supranuclear lesion, often cortical or internal capsule on the opposite side.
Q6. A patient loses vibration sense in both feet but retains pain sensation. Which major pathway is more affected?
Answer guidance: The dorsal column pathway.
Analysis
Q7. Compare an epidural hematoma with a subdural hematoma anatomically.
Answer guidance: Epidural lies between skull and dura, often arterial; subdural lies beneath dura, often due to bridging veins.
Q8. Why is lesion localization easier when deficits are grouped into motor, sensory, cranial nerve, and autonomic categories?
Answer guidance: Each system follows recognizable anatomical pathways, narrowing the lesion site.
FAQ
Q: Why do neurologists care so much about reflexes?
Reflexes help distinguish upper motor neuron, lower motor neuron, peripheral nerve, and spinal cord involvement.
Q: Is the cerebellum only about balance?
No. It also refines movement timing, coordination, and motor learning.
Q: Why are cranial nerves part of neuroanatomy and head-and-neck anatomy?
Because they arise from the brain or brainstem but travel through the head and neck to serve local structures.
Q: What is the simplest way to start learning localization?
Ask whether the pattern looks cortical, brainstem, spinal cord, root, plexus, peripheral nerve, or muscle.
Q: Why are crossed findings in the brainstem important?
They suggest involvement of cranial nerve structures on one side and long tracts affecting the opposite side of the body.
Quick Revision
- Neuroanatomy explains structure-based neurological localization.
- The CNS includes cerebrum, cerebellum, brainstem, and spinal cord.
- The PNS includes cranial nerves, spinal nerves, ganglia, and peripheral nerves.
- Gray matter processes; white matter connects.
- Corticospinal tract carries voluntary motor signals.
- Dorsal columns carry vibration and proprioception; spinothalamic tract carries pain and temperature.
- Meninges and CSF spaces explain hemorrhage and infection patterns.
- Internal capsule lesions can produce dense deficits.
- UMN and LMN signs help narrow lesion site.
- Vascular territories matter because stroke syndromes follow anatomy.
Related Topics
Prerequisites: Introduction to Human Anatomy and Head and Neck Anatomy.
Related Topics: Physiology, Psychiatry, Emergency Medicine, Radiology.
Next Topics: Embryology for developmental nervous system context, then later neurology-heavy Medicine sections for lesion application.